
Susan R., 53, from Baton Rouge, Louisiana, can tell you exactly which medications she has tried for vestibular migraines. Amitriptyline. Then verapamil, which made her ankles swell. Then topiramate, which her neurologist called the "gold standard." She took topiramate for fourteen months. The dizziness reduced by maybe 30 percent. The nausea stayed. The visual disturbance, that strange warping of the peripheral field when she turned her head, stayed completely.
"I had a name for what I had," she said. "That felt like progress for a while. Then I realized that having a name and having an answer are very different things."
Her neurologist was thorough. MRI: normal. EEG: normal. Vestibular function testing: intact. Balance testing: within normal limits. The inner ear was not the problem. The brain showed no lesions, no structural cause. The diagnosis by default was vestibular migraine, which is largely a diagnosis of exclusion: when the vestibular system tests normal and the symptoms match the pattern, vestibular migraine is the label that fits.
What vestibular migraine workups almost never include is a cervical spine evaluation.
Key distinction: Vestibular migraine medications address neurological and vascular mechanisms. They have no mechanism of action on cervical proprioceptors. If the dizziness originates from distorted position signals in the upper cervical spine, the medication is targeting the wrong system.
$119.99 (Was $239.98) | 30-Day Money-Back | Free US Shipping
The Distinction That Changes Everything
A vestibular migraine diagnosis requires, technically, an intact vestibular apparatus. When that apparatus is healthy, as it was in Susan's case, the dizziness must be coming from somewhere else.
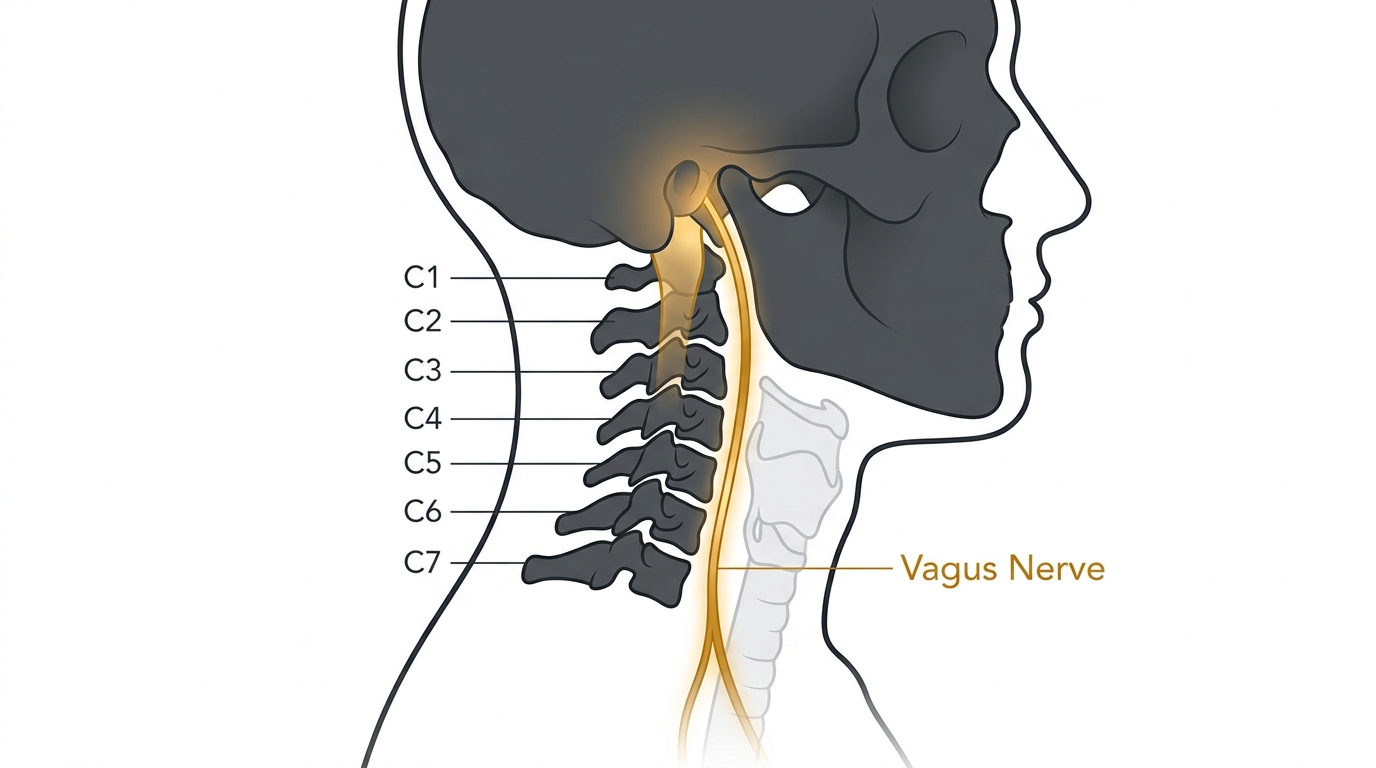
The cervical spine controls proprioception: the body's sense of its own position in space. The position sensors embedded in the muscles and joints of the upper cervical spine, particularly around C1, C2, and C3, send continuous signals to the cerebellum, the brain region that integrates balance, spatial orientation, and motor coordination.
When those cervical segments are compressed, whether from a lost cervical curve, chronic muscle tension, or an old injury that never fully healed, the position signals they transmit become distorted. The cerebellum receives conflicting information. The inner ear says one thing. The neck says another. The result: dizziness, nausea, light sensitivity, visual disturbance, a feeling of spatial unreliability. All without any inner ear problem.
Vestibular migraine medications work on brain chemistry and blood vessels. Cervicogenic vestibular dysfunction originates from distorted proprioceptive signals at C1-C3. These are different causes requiring different treatments. The symptoms look identical.
The Neurologist's Question That Never Gets Asked
Susan had five neurologist appointments over three years. She was asked about her migraine frequency, light sensitivity, sleep quality, and whether stress triggered episodes. She was never asked whether her dizziness changed when she moved her neck. She was never asked whether neck tension preceded her episodes.
"My neurologist knew everything about my brain. She knew almost nothing about my neck."
Susan R., 53, Baton Rouge, LouisianaA physical therapist who specializes in cervicogenic disorders would have asked those questions in the first ten minutes. Susan's dizziness was consistently worse after extended periods of forward head posture at her work computer. It was triggered by certain neck positions. It sometimes responded to self-massage along the back of her neck, briefly, before returning. These are not migraine patterns. These are cervical proprioceptor patterns.
What Finally Changed
Susan's sister, who works in occupational therapy, suggested she see a physical therapist experienced in cervicogenic vestibular disorders. The PT took a detailed history focused entirely on the cervical spine: posture assessment, range of motion testing, manual palpation of the suboccipital muscles and C1-C3 joints, and a lateral cervical X-ray.
The X-ray showed a significant loss of the natural cervical lordosis. The suboccipital muscles were in palpable chronic spasm. The PT explained: "Your inner ear is fine. Your cerebellum is fine. But the signals coming from your neck are telling your brain you are moving when you are not. That's the conflict."
She began cervical traction: a structured protocol of gentle mechanical decompression at C1-C3, combined with heat and manual work to address the chronic muscle tension. Over four sessions, Susan's episodes began to decrease in frequency. After eight weeks of twice-weekly sessions plus daily home traction work, her dizziness was occurring roughly once a week rather than near-daily.
"That was more progress in eight weeks than three years and three medications had given me."
Susan R., 53, Baton Rouge, LouisianaWhy the Medications Never Fully Worked
Amitriptyline, verapamil, and topiramate all address neurological or vascular mechanisms of migraine. They have no mechanism of action on cervical proprioceptors. They cannot correct the distorted position signals coming from a compressed C1-C2 segment.
This is not a failure of the medications. They are doing what they were designed to do. The failure is diagnostic: if the problem is cervicogenic rather than neurological or vascular, the right intervention is mechanical, not pharmaceutical.
The same symptom presentation can have two completely different causes. A vestibular migraine treated as a vestibular migraine will partially respond to vestibular migraine medication. The same presentation, caused by cervical proprioceptive dysfunction, will not.

Neckline 4-in-1 Massager
Clinical cervical traction for daily home use
- 26° cervical traction incline (decompresses C1-C3)
- Deep heat to reduce suboccipital muscle spasm
- EMS to interrupt the chronic tension cycle
- Targeted suboccipital massage
- 15-minute daily protocol
- 30-Day Money-Back Guarantee
$239.98 $119.99 Spring Sale
The Structural Fix: Cervical Traction
Cervical traction decompresses the upper cervical joints, C1, C2, and C3, that are responsible for proprioceptive signal generation. When these joints are restored toward their natural alignment and the chronic muscle tension is reduced, the distorted signals normalize. The cerebellum receives consistent, accurate position information.
The Neckline 4-in-1 Massager provides the core mechanical action of clinical cervical traction for daily home use. The 26-degree cervical traction incline creates gentle axial decompression of the upper cervical joints. Deep heat therapy reduces the chronic muscle tension in the suboccipital muscles. EMS interrupts the spasm cycle. The massage function targets the suboccipital triangle, the specific muscle group most associated with cervicogenic vestibular symptoms.

Susan's Results: Week by Week
Susan R. — Progress Timeline
What Users Are Saying
"I was diagnosed with vestibular migraines at 51 after two years of near-constant dizziness. Tried three different medications. They helped but never enough. My occupational therapist friend suggested cervicogenic dysfunction might be worth investigating. I started cervical traction and used the Neckline for daily home sessions. Eight weeks later my episodes went from 15 to 20 per month to maybe four or five."
"The vestibular migraine diagnosis felt like an answer. After two years on medication that mostly managed things but never fixed them, I started asking more questions. A physical therapist finally looked at my neck X-ray and pointed to the missing curve. Cervical traction made more difference than anything the neurologist prescribed. The Neckline is how I maintain it daily between PT appointments."
"I had vestibular migraines for six years. Three medications, two neurologists, one ENT. Nobody looked at the cervical curve until a PT caught it on an X-ray. I have been using the Neckline for four months and my episodes are maybe 20 percent of what they were. I wish someone had looked at this years ago."