
The headache starts the way it always does for Sandra K., 53, of Columbus, Ohio.
Not dramatic. Not sudden. It builds from somewhere at the base of her skull, works its way forward, and arrives behind her left eye like a slow tide coming in. By 9 a.m. on a Tuesday, she has already taken the pill, drawn the curtains in the spare bedroom, and told her husband she won't be at dinner.
Sandra had been seeing neurologists for six years.
Scroll for the full story, or check current availability for the at-home device that addresses the structural cause many headache specialists miss:
See If It's Still AvailableThe Appointment That Always Ended the Same Way
Sandra's first neurologist was in 2017. He was thorough: ordered an MRI, ran bloodwork, checked her eye pressure. Everything came back normal. He wrote her a prescription for sumatriptan, handed her a printed pamphlet about migraine triggers, and told her to keep a headache diary.
She kept the diary for eight months. The headaches kept coming.
The second neurologist ordered a lumbar puncture to rule out elevated intracranial pressure. It was one of the most uncomfortable procedures she had ever experienced. The result: normal. He added a daily prophylactic, topiramate. It made her word-retrieval slower. It did not meaningfully reduce the headaches.
The third specialist, a headache clinic neurologist, suggested Botox injections. Sandra had heard this worked for some people. She completed two rounds, 31 injections each, spaced twelve weeks apart. She kept a careful log. The frequency went from roughly eighteen headache days per month to fifteen.
Three doctors. Four medications. One injection procedure. Six years.
Nobody, in six years, had pressed their fingers anywhere near her neck.
What Sandra Actually Had
The morning that changed the trajectory of Sandra's situation was not at a neurologist's office. It was at a physical therapy clinic in Westerville, Ohio, where she had been referred for unrelated shoulder stiffness after a minor car accident.
Her therapist, a PT named Aaron, watched her walk in. She held her head slightly forward. Her chin protruded about two centimeters ahead of where it should be relative to her spine. He asked, before she had even described her shoulder, whether she had headaches.
She looked at him.
He sat her down, placed his thumb just below the base of her skull, at the junction of C2 and C3, and applied gentle sustained pressure.
The familiar pressure behind her left eye began to fade within three minutes.
"Nobody ever did that before," she said.
"Nobody ever looked here," he said.
Why C2 and C3 Send Pain to Your Forehead
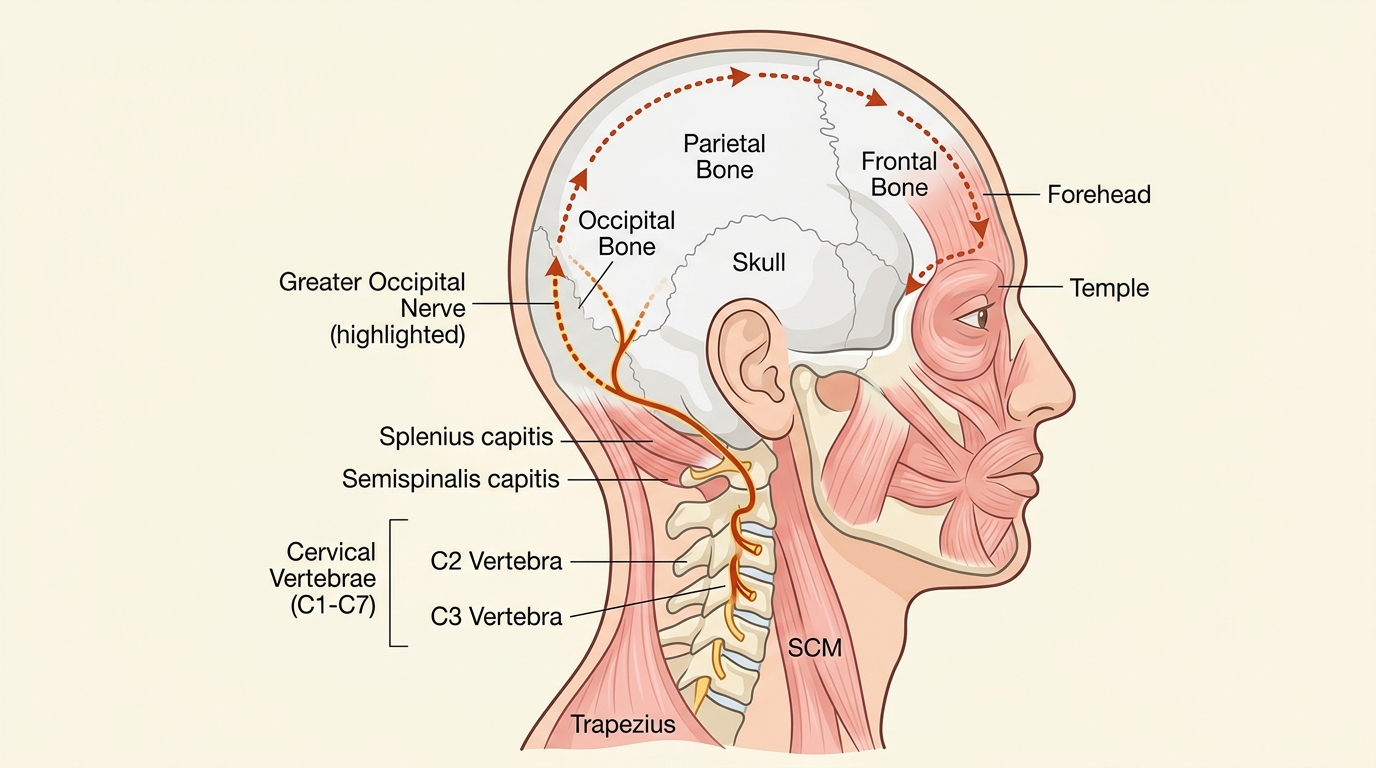
The cervical spine has eight nerve root levels. The ones that matter for understanding Sandra's headaches are the second and third: C2 and C3.
The C2 nerve root gives rise to the Greater Occipital Nerve. This nerve runs upward from the base of the skull, pierces through the suboccipital muscles, and travels directly to the scalp, the forehead, and the area behind the eye. When the soft tissue around C2 and C3 is inflamed, thickened, or under sustained compression, the Greater Occipital Nerve carries that irritation forward along its entire path.
The result is pain at the forehead, temples, and behind the eye. The same pain pattern produced by a classic migraine.
On a brain MRI, there is nothing to see. There is no vascular change, no structural brain abnormality, nothing to explain the pain. Because the origin is not in the brain. It is two inches lower.
The clinical term is cervicogenic headache: headache originating from the cervical spine. Research published in Cephalalgia, the leading international headache journal, documents that up to 20% of patients carrying a chronic migraine diagnosis may have a cervicogenic component. Many of these patients have spent years pursuing treatments directed entirely at the wrong location.
Why Migraine Medications Did Not Work
Triptans, the medication class that includes sumatriptan, work by constricting blood vessels in the brain and blocking pain receptor activity in the trigeminal nerve pathway. That mechanism is specifically designed for vascular migraines: headaches caused by brain chemistry and blood vessel behavior.
Cervicogenic headache has nothing to do with brain chemistry. It is a structural problem. The C2 nerve root is being irritated by the tissue and joint structures directly surrounding it. No oral medication crosses into that compressed tissue space in a meaningful way. No triptan reaches a nerve root.
This is why the medications help some people and not others. The ones they help are the ones with true vascular migraines. The ones they do not help are often the ones with cervicogenic involvement.
Prophylactic medications like topiramate work by broadly reducing neurological excitability. They can reduce the intensity of any headache, regardless of origin. They do not address the structural cause. When you stop them, nothing has changed.
The Botox pattern: For the subset of patients where Botox partially works for headache, the mechanism is probably muscle relaxation around the suboccipital region. It is an accidental partial solution applied without knowing why it sometimes helps. The injection sites at the base of the skull are the ones closest to the actual problem.
The Structural Problem: What Is Actually Happening in the Neck
In cervicogenic headache, the suboccipital muscles, the small deep muscles at the base of the skull, are in chronic low-grade contraction. This sustained tension gradually compresses the C2-C3 joint space. The surrounding tissue becomes inflamed. The Greater Occipital Nerve, which passes through this tissue, becomes sensitized.
In most people, this compression develops slowly over years. A forward head posture, the kind that develops from a desk job, from driving, from looking at a screen for eight hours a day, shifts the center of gravity of the head forward. For every inch the head moves forward from neutral position, the effective weight the cervical spine bears increases significantly.
Over time, the suboccipital muscles, working constantly to hold the head up, never fully release. The tissue thickens. The joint space narrows. The nerve becomes increasingly irritated.
The neurologist looking at the brain on an MRI is looking at the correct place for vascular migraines. There is nothing wrong with the approach for true migraines. The problem is that the same symptom pattern, the same forehead pain, the same light sensitivity, the same nausea, can also be produced by cervicogenic compression. And that source never shows on a brain scan, because the brain is fine.
The Two Things That Need to Happen
Aaron, the physical therapist, explained to Sandra what needed to occur for the headaches to stop.
First, the compressed joint space at C2-C3 needed to be opened. In clinical settings, this is done with cervical traction: a controlled, sustained pull along the axis of the spine that gently separates the vertebral segments and allows the inflamed tissue to decompress. In a physical therapy office, this is done with a traction device or manually.
Second, the suboccipital muscles needed to be forced to release. They had been in chronic contraction so long they had essentially forgotten how to relax on command. The EMS protocol, electrical muscle stimulation applied to the suboccipital region, forces an involuntary contraction-and-release cycle in the muscles, breaking the pattern.
Heat applied to the region increases local blood flow and accelerates the removal of inflammatory byproducts from the compressed tissue.
"How often would I need to come in?" Sandra asked.
"If you were doing this at home," Aaron said, "fifteen minutes a day would be enough."
The At-Home Device That Does All of This
The Neckline 4-in-1 Massager was designed to deliver the same mechanical interventions Sandra's physical therapist described, without the office visit.

The device creates a 26-degree cervical traction incline, the same angle used in clinical cervical traction protocols, to gently separate the C2-C3 joint space and allow compressed tissue to decompress. You lie down. Gravity does the work.
The built-in EMS function delivers electrical muscle stimulation to the suboccipital and surrounding cervical muscles, forcing the contraction-and-release cycle that releases chronic tension. The muscles do not get to stay contracted. They have to let go.
The deep heat function raises local tissue temperature, drawing increased blood flow to the compressed area and helping the inflammatory cycle resolve.
The fourth function, cervical massage, addresses the broader muscle tissue surrounding the treatment area.
The protocol is fifteen minutes. You lie down with the device. You stand up with a neck that has been mechanically decompressed.
Featured Product
Neckline 4-in-1 Massager
Cervical traction + EMS + deep heat + massage. 15 minutes a day.
- 26-degree cervical traction incline (C2-C3 decompression)
- EMS: forces suboccipital muscle release
- Deep heat: increases blood flow to compressed tissue
- Cervical massage: full surrounding muscle relief
- 15-minute daily protocol
- 30-Day Money-Back Guarantee
- Free US Shipping
Limited stock at this price
Sandra's First Six Weeks
Sandra purchased the Neckline device in early October. Aaron had explained what to expect.
Week 1: The first three sessions produced significant soreness in the suboccipital region, which Aaron had told her to expect. The muscles were releasing for the first time in years and responding to EMS stimulation they had never experienced. On the morning of day six, she woke up without a headache. It was the first headache-free morning she could clearly remember in over two years.
Week 3: The frequency of headaches had dropped noticeably. She was still having some, but the onset was slower, less severe, and responding better when it did arrive. She had not used sumatriptan in eleven days. She returned to work full days without scheduling around the possibility of a headache.
Week 6: Sandra spoke with her primary care physician about the prophylactic medication, topiramate. Her physician agreed to a supervised taper. She reduced the dose over four weeks and stopped entirely.
Always consult your doctor before making any changes to prescription medications. Sandra's experience reflects her individual results, which are not typical or guaranteed.
She still uses the Neckline device three to four times a week.